A 71-year-old female presented with dysphagia, intermittent left upper abdominal pain, and unintentional weight loss of approximately 7 lbs. over 4 months. (pdf link below)
An abdominal CT scan with contrast demonstrated an 8.5 x 6.0 x 5.5 cm solid, well-marginated mass along the fundus of the stomach, extending to the gastroesophageal junction (Figure 1). Upper gastrointestinal endoscopy showed a large subepithelial gastric mass with no bleeding or ulceration of the mucosa located in the cardia/fundus of the stomach (Figure 2). EUS revealed a hypoechoic subepithelial gastric mass in the cardio-fundic region which appeared to originate from the muscle layer of the stomach wall. Fine needle aspiration and biopsy were performed (Figure 3) followed by a proximal gastrectomy. The gross photo and microscopic findings are shown below (Figure 4-5).

Abdominal CT scan demonstrating an 8.5 cm solid, well-marginated mass with non-homogeneous contrast enhancement along the fundus of the stomach extending to the gastroesophageal junction.

Endoscopic picture of intact gastric mucosa with bulging subepithelial mass in the cardia/fundus of the stomach visible on retroflexion view.
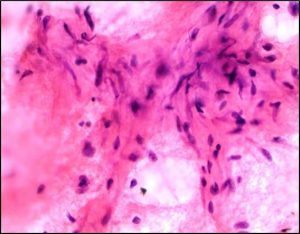
3A: FNA of submucosal lesion showing a few aggregates of cytologically bland spindle cells with myxoid background.
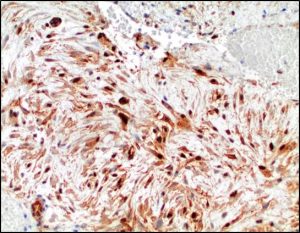
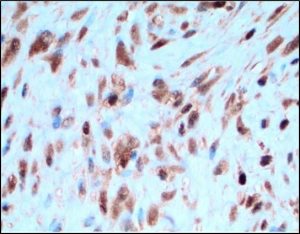
3B: Immunohistochemical stain for β-catenin shows strong and diffuse nuclear and cytoplasmic labeling in the tumor cells.

Cross section of the resected gastric mass reveals a well-demarcated intramural heterogenous mass with discrete contours. The overlying mucosa (upper portion of the picture) and the serosal surface (lower portion of the picture) are both intact. Esophageal-gastric junction is on the left side of the picture.
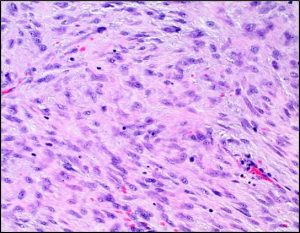
5A: High-power view of the central area of the lesion demonstrating a hypercellular storiform pattern of spindle cells with moderate nuclear pleomorphism and inconspicuous nucleoli.

Intermediate-power of hypocellular area from the periphery of the mass demonstrating spindle cells in a myxoid background containing dilated blood vessels with a staghorn pattern.
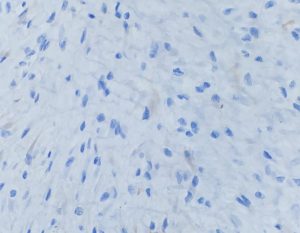
5C: Immunohistochemical stain for CD117 is negative.
5D: Immunohistochemical stain for β-catenin shows cytoplasmic and strong nuclear labeling in the tumor cells.